| ELIGIBILITY (Admin-only) |
|
|---|---|
| Parent/Guardian First Name: | Porisha |
| Parent/Guardian Last Name: | Jones |
| Parent/Guardian Cell Phone: | 7573815648 |
| Email: | porishajones@gmail.com |
| Player Information | |
| First Name: | Tremaine |
| Last Name: | Stevens |
| Child Date of Birth | 12/02/2010 |
| JERSEY NUMBER | 50 |
| School: | Oscar Smith Middle |
| Grade: | 7 |
| Address: | 2011 Chesapeake Drive |
| City: | Chesapeake |
| State: | Virgina |
| Zip / Postal: | 23324 |
| Upload Player Headshot |  |
| Upload Government Issued ID | 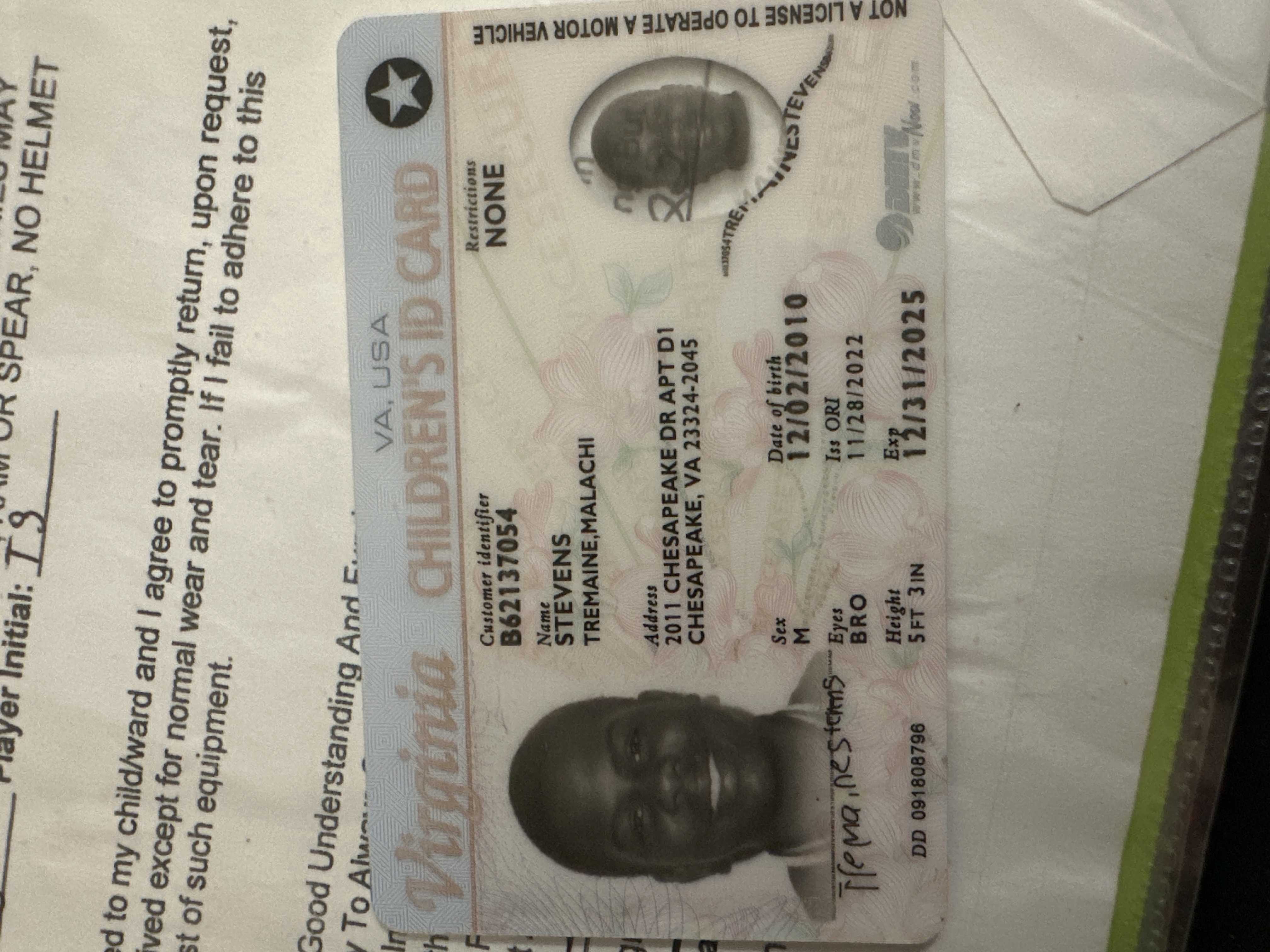 |
| Emergency Contact | |
| Primary Emergency Contact Name: | Charline Jones |
| Primary Emergency Contact Phone Number: | 7579560637 |
| Primary Emergency Contact Relationship to Player: | Aunt |
| Medical History | |
| UPLOAD PROOF OF PHYSICAL | 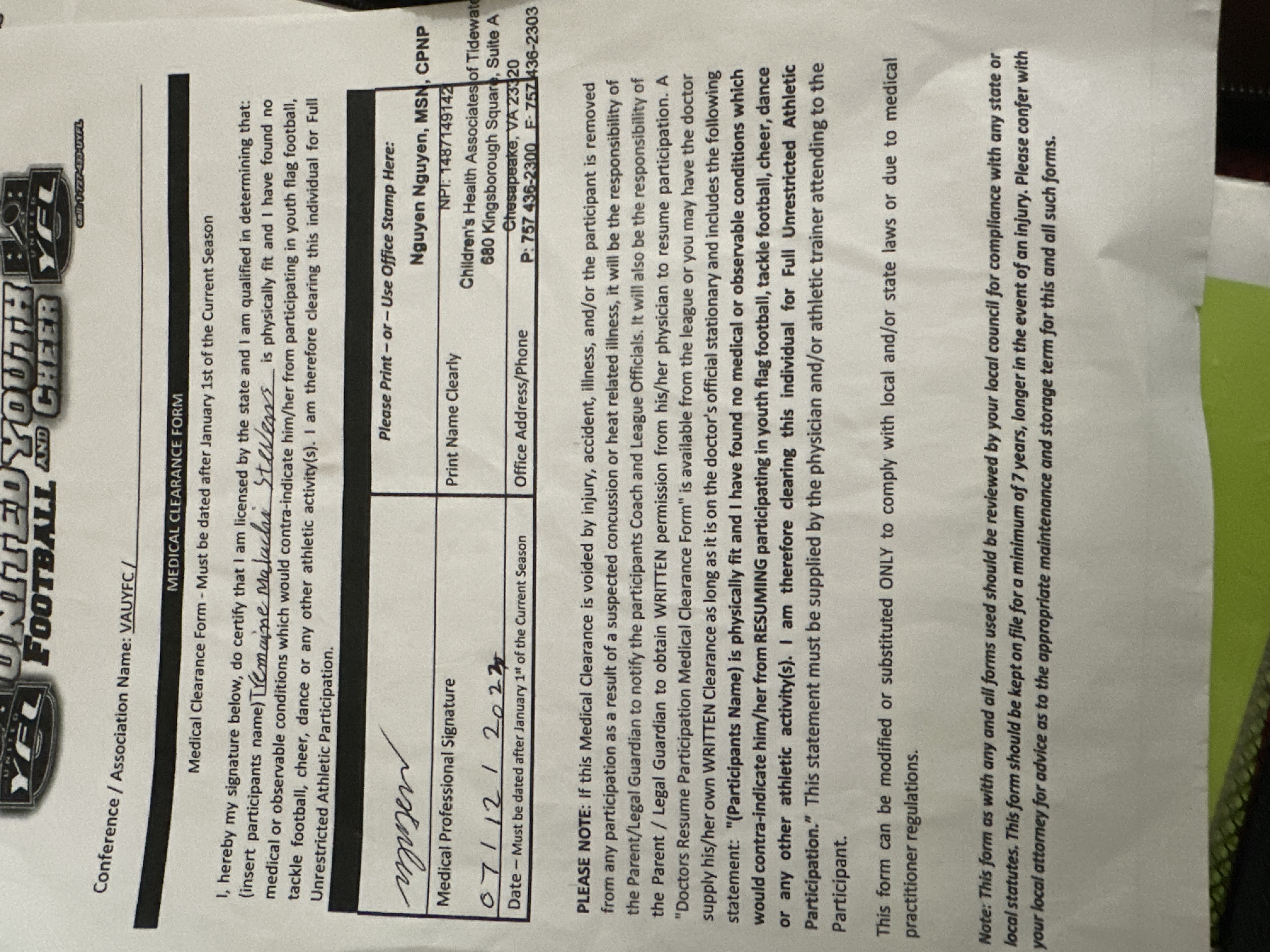 |
| Does the player have any allergies that we need to be aware of? * | No |
| Does the player have any other medical conditions that we need to be aware of? * | No |
| REGISTRATION | REGISTRATION, Qty: 1, Price: $15.00 |
| Payment Method | PayPal Checkout |
